
Increased Homocysteine Levels – A Possible Cause of Many Diseases
Despite having been deemed the “new cholesterol”, most people have never even heard of homocysteine. Even so, in the medical world this amniotic acid is at the forefront of attention, having been found to be involved in the onset of numerous diseases. An elevated homocysteine level is associated with damage to the blood vessels and can therefore lead to high blood pressure, heart attacks and strokes (1, 2). Moreover, too much homocysteine has a negative effect on cell health, which has been linked to dementia and Alzheimer’s disease (3). Further links with depression, eye disorders and osteoporosis are still being researched.
So far, only about 50% of heart attacks and strokes can be medically explained, which is why new risk factors are under intense investigation. Homocysteine is currently one of the most likely candidates; it is currently assumed that about 10% of heart attacks and strokes are due to elevated homocysteine levels (4, 5).
High concentrations of homocysteine directly damage the cells, which is why it is referred to as a cell poison. This label is somewhat misleading, since homocysteine is a necessary and natural intermediary substance in the metabolism; at the same time, it leads to a thickening of the blood and so – from two directions at once – contributes to an increased cardiovascular risk (6).
Homocysteine and the Vitamin B12 Supply
Normally, homocysteine is an intermediate product of the metabolism, which accumulates in the cells and is further processed into other substances – for example, the vital S-adenosylmethionine (SAM), which is the basis for the synthesis of many health-relevant substances. However, for the metabolic steps that convert homocysteine, vitamin B12 and folic acid are required; if these vitamins are missing, homocysteine cannot be further utilised and gets stuck in a dead end. Homocysteine thus accumulates and at a certain level becomes critical for health.
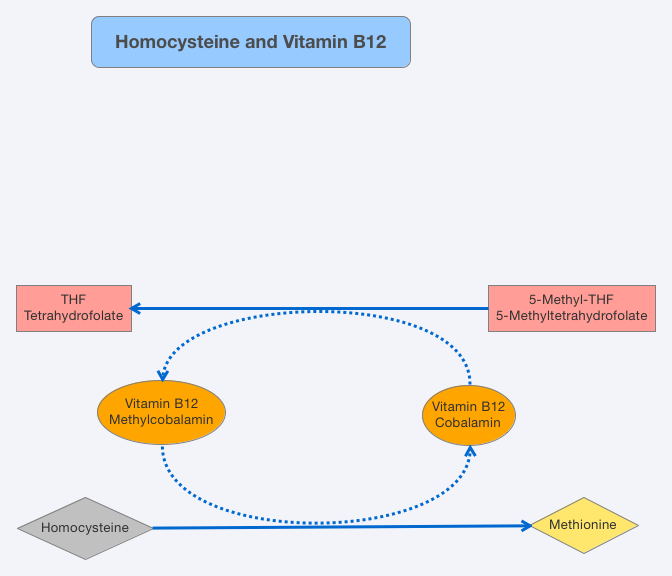
In addition to this, with the help of betaine, homocysteine can be converted into methionine in a second metabolic pathway in the liver and kidneys; or, with the help of vitamin B6, it can be degraded into cysteine. The critical factors for homocysteine levels are therefore betaine and vitamin B6 – as well as, most importantly, vitamin B12 and folic acid.
Homocysteinemia – An Indicator of Vitamin B12 Deficiency
Due to the close correlation between high levels of homocysteine and vitamin B12 deficiency, the former is frequently used as an indirect indication of the latter. Elevated homocysteine levels, also known as homcysteinemia, often signpost B12 deficiency – although the absence of folic acid may also be a cause. Since measuring B12 in the blood serum is highly unreliable, homocysteine levels are often also calculated in tests in order to better interpret results.
Homocysteine Values
The homocysteine values required for diagnosis are measured in the blood. Below are the common interpretations of these values:
Interpretation | Homocysteine value µmol/L |
Normal value | < 8 -10 |
Increased value | 10 – 12 |
Critical value (urgent treatment needed) | > 12 |
The Homocysteine Level: Risks for Older People and Vegans
High homocysteine levels are particularly common in elderly people and vegans; the cause is often a lack of vitamin B12. While the vegan diet naturally contains very little B12, it is mainly absorption disorders that cause a deficiency in older people. About 40-60% of older people have increased homocysteine levels.
If you consume a lot of alcohol and/or coffee, take certain medications and suffer from stomach, intestinal or liver diseases; you are also at risk of high homocysteine levels. Further details can be found in our vitamin B12 deficiency charts.
Homocysteine – Only an Indicator?
The assessment of homocysteine as a risk factor in the onset of diseases is also viewed critically. For example, Norbert Fuchs argues that homocysteine is not itself the cause of diseases, but only the indicator of a nutrient deficiency. Hence, he believes that it is the underlying nutrient deficiency that is the real problem (7). Homocysteine merely indicates a disturbance in methyl group transfer, which is of major importance in the formation and regeneration of new cell structures, haematopoiesis, cardiovascular metabolism and the synthesis of neurotransmitters.
Arguably, the substances involved in this context – choline, betaine, vitamin B6, vitamin B12 (methylcobalamin), folate (methyl-THF) and SAM – all have a much more direct connection to the symptoms attributed to homocysteine and are therefore often the root cause of a disease. A reduction of homocysteine is therefore a short-sighted solution; instead, the supply of nutrients should be measured, controlled and optimised.
On the other hand, some recent studies do indicate the direct causal involvement of homcysteinemia in the onset of various diseases.
- For more information, see: Homocysteine Levels: The Risk of High Homocysteine
Homocysteine Levels Decrease with Vitamins
Whether homocysteine is just an indicator or a harmful substance itself is still under investigation. Regardless, the best precaution against high homocysteine levels and possible nutrient deficiencies is maintaining a sufficient, balanced supply of vitamins. B12 and folate deficiencies are exceedingly widespread; whereas vitamin B6 or betaine are required less by the body.
In addition to the usual vitamin B12 supplements, there are now also special combination supplements that are tailored to the reduction of homocysteine and contain all relevant nutrients. Whether such supplements are actually required can first be determined by a simple blood test. In any case, vegans/vegetarians and elderly people in particular should pay close attention to their B12 supply; usually a simple B12 supplement is enough.
Sources
- Fanapour PC, Yug B, Kochar MS. Hyperhomocysteinemia: an additional cardiovascular risk factor. WMJ. 1999 Dec;98(8):51-4. Review. PubMed PMID: 10639897.
- van Beynum IM, Smeitink JA, den Heijer M, te Poele Pothoff MT, Blom HJ. Hyperhomocysteinemia: a risk factor for ischemic stroke in children. Circulation. 1999 Apr 27;99(16):2070-2. PubMed PMID: 10217643.
- SESHADRI, Sudha, et al. Plasma homocysteine as a risk factor for dementia and Alzheimer’s disease. New England Journal of Medicine, 2002, 346. Jg., Nr. 7, S. 476-483.
- Christine Vetter. Homocysteinämie – Risikofaktor für Herz und Gefäße. Zahnärztliche Mitteilungen 23/2003
- Stanger O, Herrmann W, Pietrzik K, Fowler B, Geisel J, Dierkes J, Weger M; DACH-LIGA Homocystein e.V. DACH-LIGA homocystein (german, austrian and swiss homocysteine society): consensus paper on the rational clinical use of homocysteine, folic acid and B-vitamins in cardiovascular and thrombotic diseases: guidelines and recommendations. Clin Chem Lab Med. 2003 Nov;41(11):1392-403. Review. Erratum in: Clin Chem Lab Med. 2004 Jan;42(1):113-6. PubMed PMID: 14656016.
- Guilland JC, Favier A, Potier de Courcy G, Galan P, Hercberg S. [Hyperhomocysteinemia: an independent risk factor or a simple marker of vascular disease?. 1. Basic data]. Pathol Biol (Paris). 2003 Mar;51(2):101-10. Review. French. PubMed PMID: 12801808.
- Norbert Fuchs. Homocystein – Risikofaktor, der keiner ist. PharmaTimes, 04/2011

