
- How do vitamin B12 and folic acid work together?
- What is the difference between folate and folic acid?
- What is methylation and what is an MTHFR mutation?
Vitamin B12, Folic Acid and Homocysteine
Vitamin B12 and folic acid (also folate, vitamin B9) are very closely connected in the metabolism. Both play an important role together in the methylation cycle and the formation of S-adenosylmethionine (SAM), the most important methyl donor in the human body. Vitamin B12 and folic acid are joint cofactors of methionine synthesis: the conversion of harmful homocysteine into methionine.
Vitamin B12 is responsible for reactivating folic acid, by converting it through various reactions back into tetrahydrofolate, the form of folic acid which the body can use. The metabolism of folic acid takes place in a continuous cycle, in which folic acid passes through various forms that have different effects.
A deficiency of vitamin B12 leads to an indirect, functional folic acid deficiency, as the lack of the former interrupts the cycle of the latter. Even if enough folic acid is present in the body, without B12 it cannot fulfil many of its functions because it is “stuck” at a certain point in its cycle (1, 2).
On the other hand, vitamin B12 cannot fulfil its role in the deconstruction of homocysteine without folic acid; the two vitamins are dependent on one another. Before we explore this relationship in further detail, it is important to first take a look at the most important information regarding the role of folic acid in the body.
Folic Acid and Folate
Folic acid is a synthetic compound which cannot be directly utilised by the body. The natural and bioactive form of folic acid is folate, which is used in various chemical forms in the body. Folic acid is not bioactive – therefore, it must be converted into folate first, in order to fulfil its function as an enzyme (3).
The form of folate that is genuinely bioactive, which circulates in the blood and can be absorbed in the cells, is called L-5-methyltetrayhydrofolate (L-5-MTHF) or – for the sake of simplicity – methylfolate. Normally, the body is able to absorb folic acid and convert it into folate. However, since this is not always the case, supplements are now also available that directly contain bioactive L-5-MTHF.
The two most effective active ingredients are metafolin and quatrefolic, which supply the active form L-5-MTHF (L-5-Methyltetrahydrofolate) directly. Quatrefolic has the best bioavailability.
It is estimated that around 25% of the population worldwide have a genetic mutation, which impedes the conversion of folic acid into methylfolate among other things. Known as an MTHFR mutation, we will discuss this topic in more detail later in this article.
Since the term “folic acid” has unfortunately prevailed in vernacular speech to mean “folate”, despite the large chemical differences, in the following we will use the two synonymously and will only distinguish when it comes to specific forms.
Key Points
|
Find Combination Supplements Online
| Dose B12/folate | Active ingredient – folate | Active ingredient – B12 | Online search |
| 1000 µg/400 µg | Quatrefolic | Methyl-, adenosyl- and hydroxocobalamin | Vitamin B12 + methylcobalamin + adenosylcobalamin + 1000 µg + quatrefolic folate + 400 µg |
Vitamin B12 Deficiency Causes Folic Acid Deficiency
Since a lack of vitamin B12 also leads to a folic acid deficiency, the former has a doubly important position in the cell metabolism. Both vitamins fulfil important functions and are essential for maintaining health. Folic acid is responsible for the following tasks:
- Cell division
- Haematopoiesis (blood formation)
- Formation of the mucosa
- DNA synthesis
- Protein metabolism
- Fat metabolism
A lack of folic acid can hence lead to many severe symptoms, such as anaemia, depression, gastrointestinal problems and weight loss.
Folic Acid and Pregnancy
The most serious consequences of a folic acid deficiency can be seen during pregnancy. Here it can lead to miscarriage, malformations, premature birth, heart defects and development disorders (4).
Folic acid plays a vital role in the development of the neural tube – the first development stage of the nervous system – as well as in cell growth processes and in DNA synthesis. Plus, folic acid is also the only vitamin that can prevent spina bifida.
Pregnant women in particular should ensure that they maintain a good supply of folic acid and vitamin B12 (5).
The daily requirement for folic acid almost doubles in pregnancy and is difficult to meet through a normal diet, which is why folic acid deficiencies are especially common here. In most cases, gynaecologists recommend taking supplements containing 400 – 800 µg of folic acid per day during pregnancy.
Whilst breastfeeding, the body’s requirement for folic acid also remains high. It is therefore advisable to take supplements at this time as well.
Folic Acid and Conception
Women who are trying to conceive should be sure to check their folic acid supply before pregnancy begins. Often women who become pregnant remain unaware that they have conceived for the first two to four weeks, before they are able to confirm pregnancy with an over-the-counter test. This period of time, however, is a critical phase for the development of the embryo, during which folic acid is urgently needed.
Consequently, folic acid supplies should be optimal from the moment that the decision to try for a child is made. In this way, a folic acid store is already being built up, through which a stabile folic acid status can be ensured during pregnancy.
However, the rumour that folic acid increases the chance of conception is not true.
Folate Daily Requirement
According to the Institute of Medicine (IOM, now the National Academy of Medicine), the requirement for folate is 400 µg per day for adults and 600 µg for pregnant women (6).
Age | Daily requirement (µg) |
1-3 /4-8 years | 150/200 |
9-13 /14-18 years | 300/400 |
Adults | 400 |
Pregnancy | 600 |
Lactation | 500 |
Folic acid deficiency is one of the most prevalent deficiencies. As a result, some experts have called for a legally-regulated, general fortification of foods with folic acid. Since blood values in larger studies did not indicate a critical deficiency in the general population, however, there is currently no reason to do so (5).
Folic Acid Test – Blood Levels
A person’s supply of folic acid can be checked through a blood test. Here, the total folate – i.e. the sum of different folate forms – is measured. Alternatively, the folate in the red blood cells (known as the RBC folate) can also be measured.
Here are the common reference values:
| Interpretation | Serum folate | RBC folate |
| Deficiency | < 4 ng/ml | < 150 ng/ml |
| Optimal supply | 7- 15 ng/ml | ab 400 ng/ml |
| High level | > 15 ng/ml | – |
Foods Containing Folic Acid
Folic acid is heat sensitive, meaning that foods often lose a large part of their folic acid content (40-70%) during cooking. Fresh, raw vegetables, salads and herbs are thus the best sources of folic acid. Instead of boiling vegetables, it is better to stew them, through which they retain at least some of their folic acid content.
Many food charts do not factor in the loss of nutrients during cooking and thus the statistics for raw vegetables can be misleading. Red cabbage, for example, contains 100 µg of folic acid, but after cooking contains around 45 µg. From a chemical point of view, plant-based foods always contain folate – in most cases methylfolate.
Folic Acid Food Chart
The following foods contain particularly high quantities of folic acid (9):
Food | Folic acid content (µg/100g) |
Liver (beef) | 590 |
Wheat germ | 520 |
Chickpeas | 340 |
Kale (raw) | 185 |
Parsley | 150 |
Spinach (raw) | 145 |
Lamb’s lettuce | 145 |
Dried mango | 140 |
Peanuts (roasted) | 125 |
Sunflower seeds | 120 |
Leek (raw) | 100 |
Wild rice | 95 |
Oatmeal | 85 |
Camembert | 65 |
Cherries (fresh) | 75 |
Bean sprouts (tinned) | 65 |
Asparagus (cooked) | 60 |
Quinoa, amaranth | 50 |
Olives (in oil) | 50 |
Folic Acid Vitamin B12 Supplements
Due to the close interactions of vitamin B12 and folic acid, there are many supplements which combine the two. This makes sense in many cases, especially when experiencing psychological problems and/or folic acid deficiency, as well as when pregnant. There are two key factors to consider here:
- Bioactive ingredient
B12 forms: methylcobalamin, adenosylcobalamin and hydroxocobalamin
Folate: L-5-MTHF (see following section) - Sufficient dosage
At least 250 µg B12 and 200 µg folate for general supplementation
1000 µg B12 and 400 µg folate during deficiency and medical conditions
Folic Acid Active Ingredients: Bioactive L-5-MTHF
As with vitamin B12, there are various folic acid active ingredients that have been developed over time.
| Active ingredient | Alternative/brand name | Description |
| Folic acid | Synthetic, biologically inactive form | |
| L-5-MTHF | L-5-Methyltetrahydrofolat, L-5-MTHF | Biologically active form, unstable |
| (6s)-5-MTHF calcium salt | Metafolin®, Magnafolate-C®, Extrafolate-S® | Biologically active form, stabile, good availability, patented |
| (6s)-5-MTHF glucosamine salt | Quatrefolic® | Biologically active form, very stabile, very good availability, patented, 10-20 % better availability than calcium salts |
A promising and quite new development since about 2001 is the direct use of L-5-methyltetrahydrofolate (also: (6S)-5-MTHF, L-5-MTHF, L-5-Methyl-THF, L-Methylfolate, MTHF, 5-Methyl-THF, 5-MTHF) in dietary supplements. This is the natural, bioactive form of folate found in natural foods, which is transported in the blood and absorbed by cells. It is also the form that directly interacts with vitamin B12.
Methylfolate quickly oxidises when it comes into contact with the air. In order to stabilise it as an active ingredient, it must therefore be bound to certain highly soluble salts that protect the folate and only allow it to release in the stomach. Today, various calcium salts and a glucosamine salt of L-5-MTHF are available (see table above).
Calcium-L-methylfolate is mainly marketed as Metafolin® (patented by the brand Merck). In 2010, the company Gnosis succeeded in further improving the folate active ingredients with its glucosamine salt Quatrefolic®, which significantly increased stability and bioavailability (11).
In addition to the patented active ingredients, there are also numerous other affordable calcium variations. However, here it is very important to pay attention to detail: 5-MTHF occurs in two different variants, which differ in their geometric molecular structure, however only the left-turning version can be utilised by the body. This is recognisable through the prefix L or (6s), which both denote a left-turning molecule and are identical in meaning.
The patented active ingredients are characterised by their guaranteed content of 99.9% (6s)/L-5-MTHF. With imitation supplements this high purity is not always guaranteed and up to 50% of the active ingredient can be present in an unusable, right-turning form. However, there are high-quality imitations with a guaranteed high content of active (6s)/L-forms.
Quatrefolic® is today the most effective known form of L-5-MTHF and the first choice for dietary supplements.
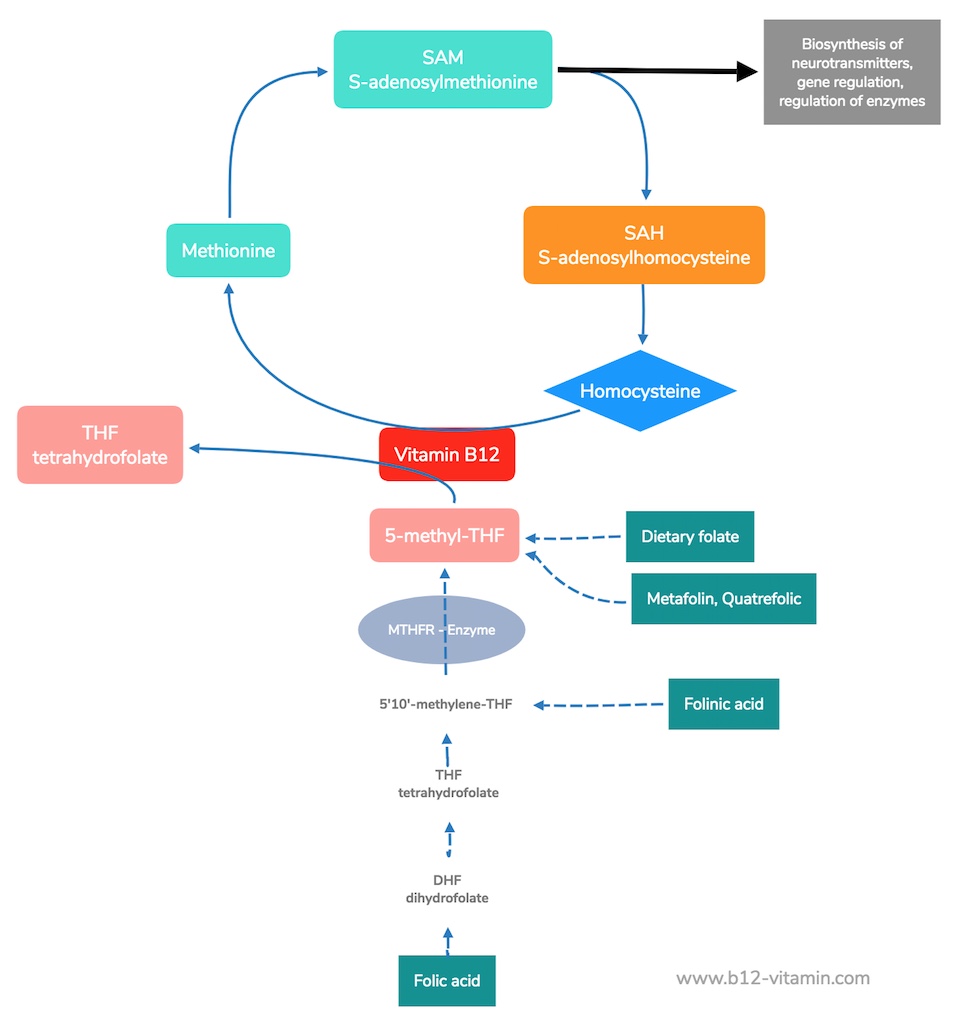
The direct administration of L-5-methylfolate makes sense, as other synthetic forms of folic acid must first be transformed into this form in many steps (see diagram below). Especially the last step of this process – the conversion of 5,10-methyl-tetrahydrofolate into L-5-methyl-THF – is impaired in many people due to enzyme disorders (MTHFR mutation), which is why the direct use of MTHF is recommended (12). The usual dosage for such supplements is between 200 and 800 µg per dose.
Folic Acid Pills, Capsules and Injections
Folic acid supplements occur most commonly in the form of pills, but capsules are also widely available. Injections are also used particularly in the treatment of anaemia patients. Capsules and injections have the advantage of being very pure in most cases, whilst pills commonly contain a variety of additives.
Folic Acid and Vitamin B Complex
Folic acid is also known as vitamin B9 and belongs to the vitamin B complex. However, since folic acid is much better known by its actual name and is often referred to as such, relatively few people are aware that it is in fact exactly the same thing as vitamin B9.
The vitamins of the B complex all work very closely together. However, vitamin B12, folic acid and vitamin B6 are particularly intertwined, all playing a role in the decomposition of homocysteine.
Folic Acid, Folate and Vitamin B12
What does the interaction between vitamin B12 and folic acid actually look like? This can be easily understood through some simple chemistry.
As previously discussed, folic acid cannot be used directly in the body; it must first be converted into various folate forms in the small intestine before absorption. The active form of folic acid found in the body is known as tetrahydrofolate (THF).
In various metabolic reactions, THF acts as a recipient and carrier of various important reaction groups such as methyl, hydroxymethyl and formyl groups. In the blood, however, folic acid circulates for the most part with a methyl group, i.e. as 5-methyltetrahydrofolate (5-methyl-THF, 5-MTHF).
With vitamin B12, this 5-MTHF now plays a kind of methyl group “ping pong”: the methyltetrahydrofolate MTHF gives its methyl group to reduced vitamin B12 (cobalamin), which then becomes methylcobalamin. At the same time, MTHF is transformed back into tetrahydrofolate by this reaction and can take on a new reaction group for further tasks.
The methylcoblamin in turn releases its methyl group to homocysteine in a further step, which converts it to methionine. Methionine is then the actual methyl group donor in the metabolism and plays an important role in the methylation of genes, proteins and lipids.
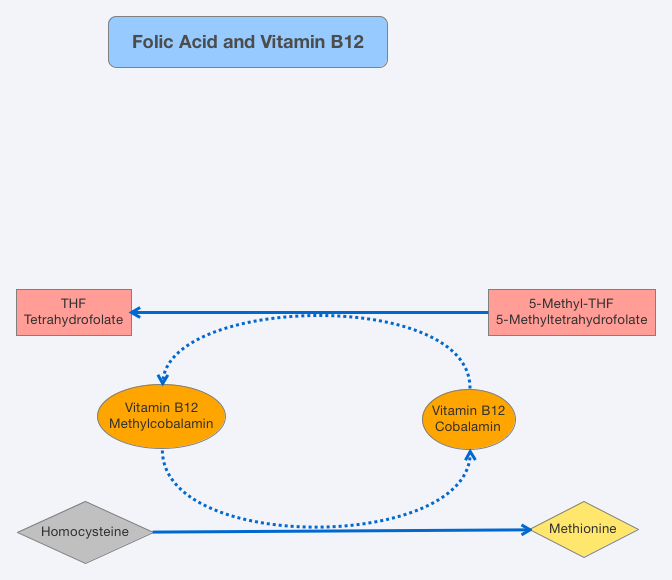
Then the cycle begins again, with the newly free cobalamin reacting with the next MTHF molecule, and so on. The result of this is twofold: firstly, the dangerous homocysteine is converted into the very important methionine; and secondly, the folic acid is regenerated. This reaction is key for many metabolic processes which are very relevant to the general health of the body.
S-Adenosylmethionine (SAM)
The methionine from this reaction is converted in further steps to S-adenosylmethionine (SAM) – one of the most important substances for the production of various neurotransmitters and for DNA methylation. The latter specifies how certain genes in the genome are selected and thus has a very profound effect on the body as a whole.
In this reaction, SAM gives off its methyl group and thus becomes homocysteine, starting the whole above-mentioned cycle once again.
Folate and Methylation
An important role for folate and vitamin B12 is their role in the methylation of SAM. As we mentioned above, SAM is the most important methyl group donors and influences a whole range of genes, chemical messengers and hormones – among many other functions.
Methylcobalamin and methylfolate are two of the most important original methyl group sources for the body and are the “recycling” point of the methylation cycle.
Methylation plays a role in almost all bodily processes, and is particularly important for controlling the genetic material (epigenetics), the production of antioxidants, the synthesis of neurotransmitters and hormones, detoxification and the immune system.
Methyl groups are passed on via the methylation cycle. Both “submethylation” – the absence of methyl groups in certain areas – as well as “overmethylation” have very noticeable, adverse effects on the body.
More information can be found in our article: Vitamin B12 and Methylation
MTHFR Mutation
Almost a quarter of the population have a gene mutation, which has negative implications for the interactions of folate and vitamin B12: what is known as the MTHFR mutation (13). MTHFR is both the name of a gene and also an enzyme. The MTHFR enzyme makes sure that L-5-MTHF is produced (see the graphic above). For people with an MTHFR mutation, the activity of this enzyme is hindered by between 30-60% (14); part of the folate is trapped.
Folic acid in this case has a correspondingly limited effect and thus people with this mutation require natural vitamin B12 and methylfolate, in order for the methylation cycle to stay intact (15).
A MTHFR mutation can only be determined through a genetic test, which is recommended by experts in the following circumstances:
- Increased folic acid levels
- High B12 levels
- Increased homocysteine levels
- Psychological illnesses
- Fibromyalgia and chronic fatigue
- Cleft palate, split spinal cord and other birth defects
Conclusion: Vitamin B12 and Folic Acid
Vitamin B12 in the forms of methylcobalamin and folate work closely together and play an essential role in the methylation cycle. Observations have shown how much both nutrients rely on each other and what an important role the chemical form can play in this interrelation.
If possible, the folate requirement should be obtained via natural foods; where this is not feasible, bioactive agents such as quadrefolic are today available.
Synthetic folic acid, on the other hand, should rather be avoided. People with an MTHFR mutation are particularly dependent on absorbing sufficient methylcobalamin and methylfolate.
Sources
- Shane B, Stokstad EL (1985) Vitamin B12-folate interrelationships. Annu Rev Nutr 5:115–141 PMID: 3927946
- Smulders YM, Smith DEC, Kok RM, Teerlink T, Swinkels DW, Stehouwer CDA, Jakobs C (2006) Cellular folate vitamer distribution during and after correction of vitamin B12 deficiency: a case for the methylfolate trap. Br J Haematol 132:623–629 PMID: 16445837
- Bailey LB (2010) Folate in health and disease. Taylor & Francis, Boca Raton
- Scholl TO, Johnson WG (2000) Folic acid: influence on the outcome of pregnancy. Am J Clin Nutr 71:1295S–303S PMID: 10799405
- Greenberg JA, Bell SJ, Guan Y, Yu Y (2011) Folic Acid Supplementation and Pregnancy: More Than Just Neural Tube Defect Prevention. Rev Obstet Gynecol 4:52–59 PMCID: PMC3218540
- Institute of Medicine, Food and Nutrition Board, National Academies of Science, Dietary Reference Intakes (DRI): Recommended Dietary Allowances and Adequate Intakes, USA 2018, http://www.nationalacademies.org/hmd/~/media/Files/Activity%20Files/Nutrition/DRI-Tables/5Summary%20TableTables%2014.pdf?la=en
- Krems C, Walter C, Heuer T, Hoffmann I (2012): Lebensmittelverzehr und Nährstoffzufuhr – Ergebnisse der Nationalen Verzehrsstudie II. In: Deutsche Gesellschaft für Ernährung (Hrsg.): 12. Ernährungsbericht 2012. Bonn 40-85
- Heseker H, Mensink GBM: Lebensmittelverzehr und Nährstoffzufuhr im Kindes- und Jugendalter. Ergebnisse aus den beiden bundesweit durchgeführten Ernährungsstudien VELS und EsKiMo. In: Deutsche Gesellschaft für Ernährung (Hrsg.): Ernährungsbericht 2008. Bonn (2008) 49-92
- Prof. Dr. Helmut Heseker, Dipl. oec. troph. Beate Heseker; Die Nährwerttabelle, 2. Aufl., 2012, Neuer Umschau Buchverlag
- http://www.merckmillipore.de/chemicals/metafolin-/c_4SOsHfETxroAAAE3QohJyIPG
- Miraglia N, Agostinetto M, Bianchi D, Valoti E (2016) Enhanced oral bioavailability of a novel folate salt: comparison with folic acid and a calcium folate salt in a pharmacokinetic study in rats. Minerva Ginecol 68:99–105 PMID: 27008238
- Pietrzik K, Bailey L, Shane B (2010) Folic acid and L-5-methyltetrahydrofolate: comparison of clinical pharmacokinetics and pharmacodynamics. Clin Pharmacokinet 49:535–548 PMID: 20608755
- Liew S-C, Gupta ED (2015) Methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism: epidemiology, metabolism and the associated diseases. Eur J Med Genet 58:1–10 PMID: 25449138
- Rozen R (1997) Genetic predisposition to hyperhomocysteinemia: deficiency of methylenetetrahydrofolate reductase (MTHFR). Thromb Haemost 78:523–526 PMID: 9198208
- Prinz-Langenohl R, Brämswig S, Tobolski O, Smulders Y, Smith D, Finglas P, Pietrzik K (2009) [6S]-5-methyltetrahydrofolate increases plasma folate more effectively than folic acid in women with the homozygous or wild-type 677C?T polymorphism of methylenetetrahydrofolate reductase. Br J Pharmacol 158:2014–2021 PMCID: PMC2807663

