
Vitamin B12 – an Essential Vitamin for the Nerves
Vitamin B12 is without doubt one of the most important vitamins for the health of the nerves. Consequently, B12 deficiency can inflict severe damage to the nerves and cause them to malfunction, which can affect in turn the cerebral cortex, nerves of the spinal cord, optic nerves and peripheral nerves in the limbs. This can result in temporary sensory and perceptual disturbances as well as permanent structural damage to the nervous system.
One of the many benefits of vitamin B12 is that it protects, develops and regenerates the nervous system and brain in a number of ways. Treatment with B12 moreover shows good results for various nervous disorders and psychological symptoms.
New research has shown that the vitamin has a hormone-like function in the nervous system and controls certain central messenger substances.
Vitamin B12 and the Nervous System
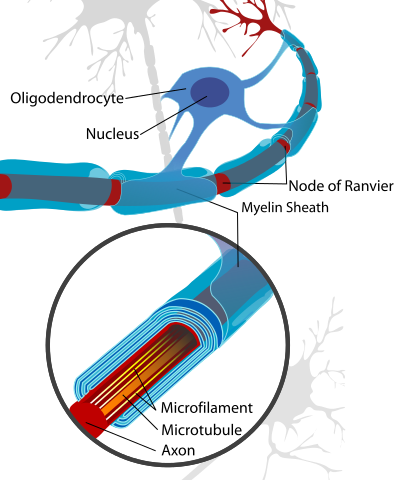
Vitamin B12 is best known for its nerve-protecting effect: it is involved in the formation of the protective layer around the nerves, known as the myelin sheath. Both the nerves in the spinal cord and the small nerve fibres of the peripheral nervous system are therefore dependent on the vitamin for maintenance.
Deficiency of B12 can therefore lead to the destruction of the myelin sheaths, triggering a range of sensations: from tingling or numbness, especially in the hands and feet, to chronic pain and irreparable paralysis. Loss of vision is also possible, if the optic nerves are affected.
In the initial stages, these symptoms can be treated very effectively with the vitamin, however a persistent deficiency can cause irreversible damage to the nerves.
Vitamin B12, the Brain and Psyche
The brain also urgently requires vitamin B12. This applies both to the development of the brain in early childhood and neural maintenance throughout life.
While vitamin B12 deficiency can lead to the underdevelopment of the brain in early life, it can also lead to severe symptoms in adulthood, ranging from dementia, memory loss and cognitive/intellectual decline; to psychosis and personality changes.
Studies have shown that a number of very different neuropsychiatric diseases and symptoms can be completely treated with B12 (1-5). An assessment of the nutrient supply is therefore urgently recommended in response to many psychiatric symptoms, as many clinical pictures can be treated with the help of dietary supplements alone. Before resorting to heavy medication, this natural treatment option should at least be taken into consideration.
Vitamin B12 and Nerves: Early Detection is Key
Even when mild neurological symptoms occur, optimising B12 levels should become a priority. The earlier B12 deficiency is recognised and remedied, the greater the chance that all symptoms can be completely eliminated through B12 therapy (6, 7).
In the case of longer-term deficiencies however there is a risk of irreversible nerve damage, which is why early detection and treatment is of utmost importance. Unfortunately, neurological practice does not always recognise the importance of vitamin B12.
For more information on detecting and diagnosing deficiency, see our article: Vitamin B12 Deficiency Test
Vitamin B12 Deficiency Symptoms in the Nervous System
B12 deficiency is associated with the following neurological symptoms. If any of these are present, a shortage of B12 should urgently be considered as a cause.
Neurological Symptoms
- Unpleasant sensations on the skin (especially on the hands and feet)
- Numbness, tingling, burning and/or a furry skin sensation
- Constant “pins and needles” in the hands and feet
- Unsteadiness when walking
- Coordination problems
- Chronic nerve pain
- Loss of vision/visual disturbances
- Paralysis
Neuropsychiatric Symptoms
- Dementia
- Cognitive disorders
- Severe concentration problems
- Depression
- Schizophrenia
- Mania
- Katatonia
- Psychosis
- Delusions
- Delirium
In this article, we will focus on neurological symptoms. The effects of B12 on the psyche are explored in depth in the article: Vitamin B12, Brain and Psyche
Vitamin B12 and Neuropathy
In advanced stages, damage to the nerves and spinal cord caused by B12 deficiency is referred to as peripheral neuropathy, polyneuropathy and funicular myelosis. However, the vitamin is also associated with other nerve diseases such as Parkinson’s disease and multiple sclerosis (8 – 10).
Another particular form of neuropathy is optical neuropathy, in which the optic nerve is attacked (11, 12). This leads to a gradual loss of vision, which can develop from visual disturbances such as spots and fogginess, to an almost complete loss of sight.
Neuropathies are often part and parcel of the symptoms of pernicious anemia (also called Biemer’s disease) – a severe form of anaemia caused by B12 deficiency. However, nerve diseases can also occur completely independently of anaemia and with a completely normal B12 blood count. Common tests for B12 can therefore give misleading results.
Blood Values are Often Misleading
It is the cellular supply of B12 that is decisive for the health of the nerves – not the blood level, which allows for only limited conclusions about the actual vitamin supply. The scientific literature contains numerous examples of nerve disorders that have been completely treated with B12 without the blood count having ever indicated deficiency (13 – 17).
More reliable is the concentration of B12 in the cerebrospinal fluid, which is almost never measured.
In the context of neurological symptoms, even the combination of holo TC, MMA and homocysteine tests can be misleading. Diagnostic values can lie in a grey area here and still problems can arise. A study conducted in 2016 thus came to the following conclusion:
“If we had restricted the treatment of symptomatic patients to patients with both low serum levels and elevated metabolite levels, 63% of patients who responded well to the therapy would not have received treatment […] Only 16% of patients with good clinical improvement from vitamin B12 therapy had low serum levels and 54% of patients with good clinical improvement from vitamin B12 therapy had serum levels higher than 300 pg/mL.”
Some experts thus advise high-dose B12 treatment to treat all known nervous symptoms associated with B12 deficiency. Especially the B12 form of methylcobalamin has proven to be very effective in many studies.
Current B12 Thresholds are Insufficient for Nerve Health
The official threshold for vitamin B12 deficiency is highly doubted in this context, as it was calculated for the prevention of anaemia. Recent research shows that the effects of vitamin B12 go far beyond haematopoiesis and that neurological and psychological symptoms typically occur at blood levels far above the current limits for B12 deficiency.
For the health of the nerves and psyche, many researchers recommend a B12 value of 600 pg/ml, which matches the official guidelines given in Japan (18).
Key Points
|
Vitamin B12 Deficiency and Nerve Damage
There are two ways in which B12 deficiency can lead to nerve damage:
- Myelinopathy: damage to the myelin sheaths (protective layer covering the nerves)
- Axonal degeneration: destruction and dying off of the nerve fibres and axons
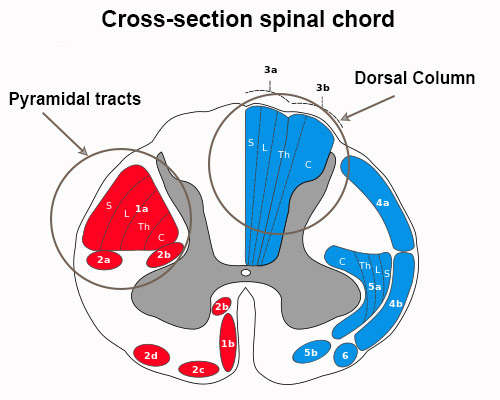
The central nerves of the spinal cord can also be affected, as well as the smallest nerve fibres in the peripheral nervous system – especially in the hands and feet.
In the spinal cord, the myelin sheaths of the nerve cords are attacked, especially in the posterior column and pyramidal tracts. In the peripheral nervous system, the death of nerve fibres has been observed (19-21).
Vitamin B12, Nerves and Myelin
Vitamin B12 is a central nutrient in the creation and maintenance of the myelin sheaths, lipid-rich protective layers which cover the nerves. On one hand, the myelin sheaths protect the nerves; on the other, they function like the isolation of an electric cable and ensure that the nerve signals are correctly transmitted.
Vitamin B12 Mechanism of Action in the Nervous System
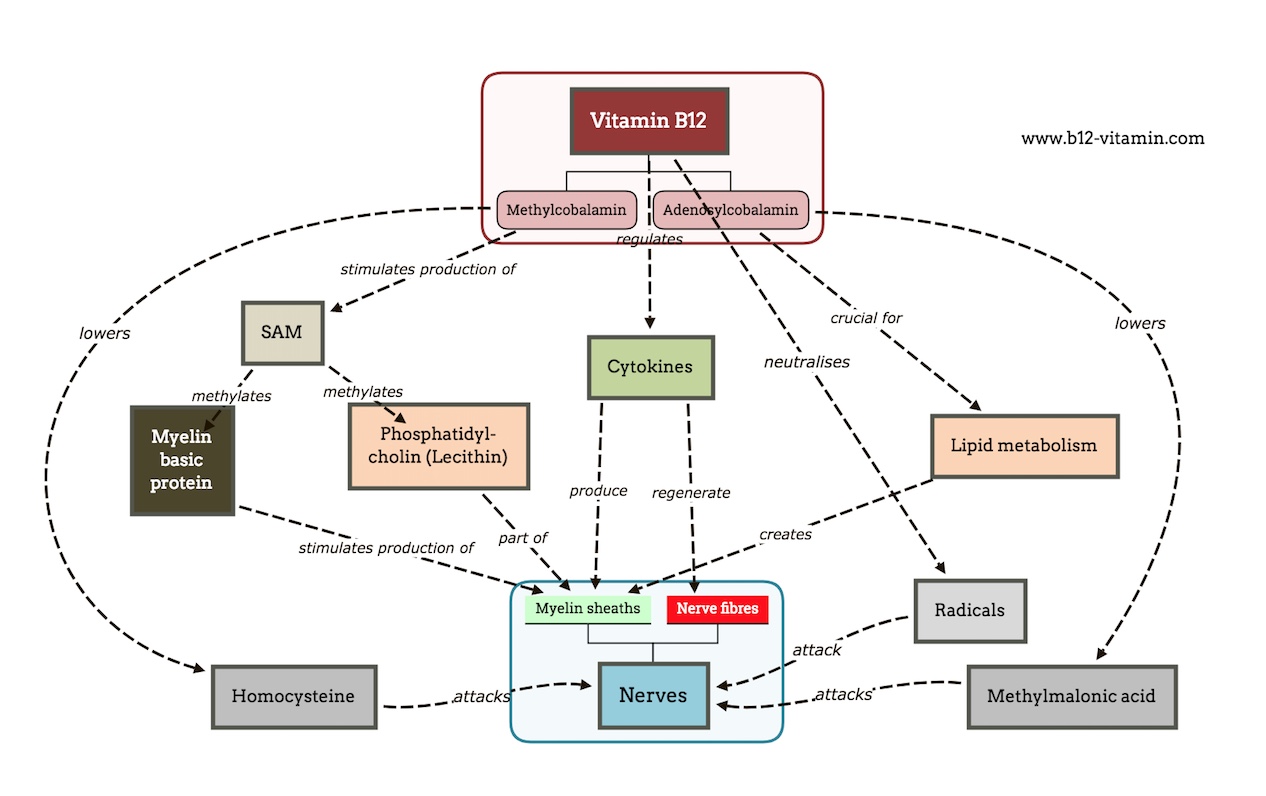
Vitamin B12 influences and regulates the creation and maintenance of the myelin sheaths through four different mechanisms:
- Required for the formation of lipids and proteins, from which myelin is created
- Lowers the level of amino acids, which are probably neurotoxic
- Works like a hormone in the central nervous system and regulates the level of important cytokines and neurotrophic factors
- Is a crucial antioxidant in the central nervous system and, through different mechanisms, protects the nerves from chronic inflammations, reactive oxygen and nitrogen radicals and toxins (22 – 24)
Vitamin B12 and the Creation of the Myelin Sheaths
Both active coenzyme vitamin B12 forms have an influence on the structure of the myelin sheaths.
Adenosylcobalamin influences the lipid metabolism. Deficiency can lead to the faulty or insufficient production of lipids, from which myelin is composed (25, 26).
Methylcobalamin is required for the creation of S-adenosylmethionine (SAM), the most important methyl donor in the human body. SAM is needed for the methylation of the myelin-based protein, which play a central role in the creation of myelin (27, 28). Methylcobalamin also promotes the formation of phosphatidylcholine (lecithin), an important component in myelin sheaths.
Vitamin B12 deficiency thus leads to the poor regeneration of and gradual damage to the myelin sheaths (29). In the primary stages this can lead to sensory disturbances and at the same time the nerves become vulnerable and can suffer severe damage.
Reduction of Homocysteine and Methylmalonic Acid
Adenosylcobalamin lowers the level of methylmalonic acid, which has nerve-destroying properties when highly concentrated (30).
Methylcobalamin lowers levels of homocysteine, which is suspected of having direct neurotoxic properties (31).
How major the effects of methylmalonic acid and homocysteine are in this context remains in question. Although both substances show nerve-damaging properties in cell experiments, it is still uncertain how much these come into effect in biological concentrations.
Vitamin B12 Antioxidant
Vitamin B12 has proven to be a very potent antioxidant that can help prevent chronic inflammation (66, 67). This mechanism of action probably plays a major role, as inflammations are causally involved in the development of nerve damage in most neurological diseases.
Here too there are several mechanisms in effect simultaneously:
- B12 is a strong antioxidant that has proven almost as potent as superoxide dismutase (oxidative stress) (68)
- B12 is a scavenger of nitrogen radicals and also controls their production (nitrosative stress) (69, 70)
- B12 plays a role in the creation of glutathione, a central antioxidant (71)
Through all of these mechanisms, vitamin B12 plays an important regulating role in all inflammatory diseases and in this way, protects the health of the nerves.
Vitamin B12 Regulates Cytokines and Neurotrophic Factors
A very new research field has brought to light astonishing new functions of B12 in the nervous system, which go far beyond its role as coenzyme and rather resemble the mode of action of a hormone: vitamin B12 regulates the level of certain neurotrophic factors – such as neurotransmitters, growth factors and the so-called cytokines – essential messenger substances that all assume a controlling function in numerous bodily processes (32).
In addition to this, vitamin B12 influences the level of prions – special proteins that are being discussed as both chemical messengers and pathogens (33).
After years of research, it has now been shown that a deficiency of the vitamin leads to an increase in myelin-damaging cytokines and a decrease in myelin-promoting cytokines (34).
Vitamin B12 therefore has a central, hormone-like effect in the nervous system.
Vitamin B12 and Nerve Regeneration
Another very new discovery is that vitamin B12 not only has an impact on the myelin sheaths, but also shows a remarkable effect in the direct regeneration of the nerves (35-37).
The exact mechanism is not yet clear. Previous research suggests that the vitamin apparently also controls important messenger substances through methylation reactions, which promote the regeneration of the nerves (38-40).
Various tests on rats were able to produce impressive results in the regeneration of a number of different nerve damages. Daily methylcobalamin injections were administered at very high doses from 500 to 1000 µg per kilo of bodyweight – this would correspond to about 40 000 – 80 000 µg per day for a human being.
There are very few experiments that have been undertaken with such dosages on humans. In the case of the currently untreatable degenerative nerve disease ALS, a daily dose of 50 000 µg of methylcobalamin via injection could significantly slow down the pace with which the disease proceeds (41).
Methylcobalamin – the Vitamin B12 Form for Nerves
Methylcobalamin accounts for up to 90% of B12 in the spinal cord and central nervous system and diffuses particularly well into neurons. This high distribution in the nervous system suggests that methylcobalamin is of central importance here, which is why methylcobalamin is the form preferred by many therapists for treating neurological symptoms.
Today, experts believe that the central workings of B12 in the nervous system are the methylation functions, production of S-adenosylmethionine (SAM) and formation of glutathione; all three activities are mainly conducted by methylcobalamin.
Nevertheless, adenosylcobalamin also appears to be involved in the formation of the myelin sheaths, which is why a combination supplement of both coenzymes is potentially most useful. Some studies have also shown good results with hydroxocobalamin, a precursor of the bioactive coenzymes that is converted into the other two coenzyme forms in the body (42).
Vitamin B12 Therapy for Neurological Symptoms: Injections or Oral Supplements?
The majority of all intervention studies on vitamin B12 and the nerves have been conducted with the use of injections; intramuscular, intravenous as well as intrathecal (directly into the spinal canal) injections have been administered (43). Due to these very divergent therapeutic applications, there is currently no general protocol for the treatment of neurological symptoms.
Treatment with injections has brought faster and better results in some comparative studies. At the same time, it has also been shown that even funicular myelosis can be successfully treated with oral B12 supplements (44).
In many other areas, oral substitution at a sufficiently high dosage has already proven to be equivalent to injections and an improvement of neurological symptoms seems to be equally possible through oral administration (45, 46).
Accordingly, the oral dose must be above 2000 µg per day even for mild symptoms. For severe nerve disorders, up to 15 000 µg per day are sometimes used. At present, there are no attempts to regenerate nerves with – however, here it would probably be useful to work with injections.
Further reading: Vitamin B12 Supplements and Vitamin B12 Dosages
Oral Vitamin B12 Supplements for Mild Nerve Disorders
The previously tested protocols for the oral treatment of nerve disorders with B12 work with multiple doses per day. This is intended to, firstly, make full use of intake via the intrinsic factor (IF) and, secondly, to lead to a constantly high B12 blood level.
Active Ingredient | Dose per Day | Administration | Duration |
Methylcobalamin | 3000 µg | 3 x 1000 µg | 6 months |
Vitamin B12 and the Development of the Nervous System
As well as being essential for the maintenance of the nervous system and brain, vitamin B12 is vital for their very formation in the first place – taking effect in the womb and throughout childhood.
Vitamin B12 deficiency in the mother during pregnancy and whilst breastfeeding, or in the child after birth, can lead to the severe degeneration of the child’s nervous system and brain (47). Especially expectant and breastfeeding mothers should pay close attention to their vitamin B12 status.
Numerous case studies report of severe impediments to the child’s development as a result of B12 deficiency in the mother (48-50). The most frequent symptoms are:
- Developmental delays
- Anaemia
- Loss of appetite
- Chronic vomiting
- Weight loss
- Low brain volume
- Spasms/cramps
- Apathy
- Irritability
In the most severe instance, vitamin B12 deficiency can lead to respiratory failures and coma (51).
This can be caused equally by the mother’s vegan/vegetarian diet or undiscovered B12 intake disorders. Keeping check of the B12 level is thus particularly worthwhile for vegans during pregnancy (52, 53).
See here:
Vitamin B12 and Child Development
While adults can tolerate an insufficient supply of B12 for quite some time without developing severe symptoms, this is not the case when it comes to children due to their lack of B12 stores in the body. If breast milk or baby food does not contain enough of the vitamin, a severe deficiency can occur within a few weeks.
While some of the developmental disorders can be compensated for over the years through an administration of B12, the few existing long-term studies indicate that intellectual abilities and other aspects of neurological development can remain permanently impaired (54).
If the B12 deficiency remains untreated for too long, damage cannot be reversed. In just over 30% of existing case studies, irreparable damage remains even after vitamin B12 therapy.
Vitamin B12 and Diabetic Neuropathy
Nerve damage is also a frequent consequence of diabetes: about one in three diabetes patients develops diabetic neuropathy. In most cases, the peripheral nerves are affected, especially those of the hands and feet. Known as peripheral sensorimotor polyneuropathy, this condition usually first occurs equally in both feet and can spread from tingling, pain and discomfort to paralysis.
More rarely affected is the autonomic nervous system, which controls the activity of the organs and other bodily functions. The most common symptoms here are heart palpitations, bladder weakness or erectile dysfunction.
The exact way in which diabetic neuropathy develops remains unclear. It is understood that a permanently increased sugar level could damage the nerves, however a B12 deficiency caused by diabetes drugs is also today a proven cause (55).
B12 is used very successfully as a therapeutic agent in diabetic neuropathy; both oral supplements and injections have proven to be effective (56 -59). Here the vitamin is somewhat more effective than painkillers or other forms of therapy (60).
These statements also apply to B12 therapy with the use of oral supplements.
Vitamin B12 and Metformin
The diabetes medicine, metformin, interferes with B12 absorption in the intestine by impeding the calcium-dependent intake mechanism. As a result, metformin patients often suffer from B12 deficiency and diabetic neuropathy (61-63).
However, this obstruction to absorption can be eliminated by taking additional calcium (64). For diabetic patients taking metformin, a combination of B12 and calcium supplements are therefore useful.
Vitamin B12 and Nerve Damage Caused by Nitrous Oxide/Laughing Gas
Nerve damage caused by B12 deficiency can also be triggered by the use of the nitrous oxide, which is frequently used by dentists.
Otherwise known as laughing gas, nitrous oxide destroys most of the B12 in the blood, cells and body stores; it can thus trigger a severe B12 deficiency. As a result, there are repeated reports of severe nerve disorders after nitrous oxide anaesthesia, which however can be remedied with B12 supplements if taken promptly afterwards (65, 66).
More information can be found in the article: Vitamin B12 Deficiency and Anesthesia
Conclusion: Vitamin B12 and Nerves
In the research into vitamin B12, nerve health is one of the central topics. What is more, the vitamin’s greatest therapeutic potential most likely lies within this field.
The significance of B12 for the nerves cannot be stressed enough. Currently, however, information on this topic is not widely circulated, which should be rectified since the vitamin can make a dramatic difference, especially for pregnant women and the elderly.
In our opinion, an assessment of the nutrient supply should always be the preliminary step in responding to all forms of neurological and neuropsychiatric symptoms. Furthermore, we consider precautionary B12 treatment to be an appropriate and advisable response to such symptoms, due to the number of positive experience reports as well as the fact that blood measurements and other test factors are often misleading in this area.
Sources
- Lachner, C., Steinle, N. I., & Regenold, W. T. (2012). The neuropsychiatry of vitamin B12 deficiency in elderly patients. The Journal of neuropsychiatry and clinical neurosciences, 24(1), 5-15.
- Lindenbaum, J., Healton, E. B., Savage, D. G., Brust, J. C., Garrett, T. J., Podell, E. R., … & Allen, R. H. (1988). Neuropsychiatric disorders caused by cobalamin deficiency in the absence of anemia or macrocytosis. New England Journal of Medicine, 318(26), 1720-1728.
- Masalha R , Chudakov B , Muhamad M, et al.: Cobalamin-responsive psychosis as the sole manifestation of vitamin B12 deficiency. Isr Med Assoc J 2001; 3:701–703
- Gomez-Bernal GJ , Bernal-Perez M : Vitamin B12 deficiency manifested as mania: a case report. Prim Care Companion J Clin Psychiatry 2007; 9:238
- Hector M , Burton JR : What are the psychiatric manifestations of vitamin B12 deficiency? J Am Geriatr Soc 1988; 36:1105–1112
- Ahmed A , Kothari MJ : Recovery of neurologic dysfunction with early intervention of vitamin B12. J Clin Neuromuscul Dis 2010; 11:198–202
- Lee WJ , Hsu HY , Wang PY : Reversible myelopathy on magnetic resonance imaging due to cobalamin deficiency. J Chin Med Assoc 2008; 71:368–372
- Miller, A., Korem, M., Almog, R., & Galboiz, Y. (2005). Vitamin B12, demyelination, remyelination and repair in multiple sclerosis. Journal of the neurological sciences, 233(1), 93-97.
- Reynolds, E. H. (1992). Multiple sclerosis and vitamin B12 metabolism. Journal of Neurology, Neurosurgery & Psychiatry, 55(5), 339-340.
- Sadasivan, S., & Friedman, J. H. (2012). Vitamin B12 (cobalamin) and Parkinson’s disease. Clinical Practice, 9(4), 353-356.
- Pineles, S. L., Avery, R. A., & Liu, G. T. (2010). Vitamin B12 optic neuropathy in autism. Pediatrics, 126(4), e967-e970.
- Chavala, S. H., Kosmorsky, G. S., Lee, M. K., & Lee, M. S. (2005). Optic neuropathy in vitamin B 12 deficiency. European journal of internal medicine, 16(6), 447-448.
- Hammond, N., Wang, Y., Dimachkie, M. M., & Barohn, R. J. (2013). Nutritional neuropathies. Neurologic clinics, 31(2), 477-489.
- Lindenbaum J, Healton EB, Savage DG, et al. Neuropsychiatric disorders caused by cobalamin deficiency in the absence of anemia or macrocytosis. N Engl J Med. 1988;318:1720- 1728.
- L. R. Solomon. Cobalamin-responsive disorders in the ambulatory care setting: unreliability of cobalamin, methylmalonic acid, and homocysteine testing. Blood 2005 105:978-985;
- Matchar DB, McCrory DC, Millington DS, Feuss- ner JR. Performance of the serum cobalamin assay for diagnosis of cobalamin deficiency. Am J Med Sci. 1994;308:276-283
- Graber JJ, Sherman FT, Kaufmann H, Kolodny EH, Sathe S. Vitamin B12-responsive severe leukoencephalopathy and autonomic dysfunction in a patient with “normal” serum B12 levels. J Neurol Neurosurg Psychiatry. 2010 Dec;81(12):1369-71.
- Dommisse, J. (1991). Subtle vitamin-B12 deficiency and psychiatry: a largely unnoticed but devastating relationship?. Medical hypotheses, 34(2), 131-140.
- Healton EB, Savage DG, Brust JCM, Garrett TJ, Lindenbaum J. Neurologic aspects of cobalamin deficiency. Medicine 1991;70: 229–45
- Bekircan-Kurt, C. E., Gunes, N., Demirci, M., Erdem-Ozdamar, S., & Tan, E. (2016). The Histopathological Evaluation of Small Fiber Neuropathy in Patients with Vitamin B12 Deficiency (P3. 154). Neurology, 86(16 Supplement), P3-154.
- McCombe, P. A., & McLeod, J. G. (1984). The peripheral neuropathy of vitamin B 12 deficiency. Journal of the neurological sciences, 66(1), 117-126.
- Alzoubi, K., Khabour, O., Hussain, N., Al-Azzam, S., & Mhaidat, N. (2012). Evaluation of vitamin B12 effects on DNA damage induced by pioglitazone. Mutation Research/Genetic Toxicology and Environmental Mutagenesis, 748(1), 48-51.
- Lee, Y. J., Wang, M. Y., Lin, M. C., & Lin, P. T. (2016). Associations between Vitamin B-12 Status and Oxidative Stress and Inflammation in Diabetic Vegetarians and Omnivores. Nutrients, 8(3), 118.M. Kikuchi, S. Kashii, Y. Honda, Y. Tamura, K. Kaneda, and A. Akaike, Protective effects of methylcobalamin, a vitamin B12 analog, against glutamate-induced neurotoxicity in retinal cell culture. Investigative Ophthalmology and Visual Science, vol. 38, no. 5, pp. 848-854, 1997
- Victor M, Ropper AH. Diseases of the nervous system due to nutritional deficiency. Adams and Victor’s principles of neurology, 7th ed. New York’ McGraw-Hill; 2001. p. 1218–22.
- Metz J. Cobalamin deficiency and the pathogenesis of nervous system disease. Annu Rev Nutr 1992; 12:59-79
- Shevell MI, Rosenblatt DS. The neurology of cobalamin. Neurol Sci 1990;19:472.
- Nishimoto, S., Tanaka, H., Okamoto, M., Okada, K., Murase, T., & Yoshikawa, H. (2015). Methylcobalamin promotes the differentiation of Schwann cells and remyelination in lysophosphatidylcholine-induced demyelination of the rat sciatic nerve. Frontiers in Cellular Neuroscience, 9, 298.
- Misra, U. K., Kalita, J., & Das, A. (2002). Vitamin B12 deficiency neurological syndromes: a clinical, MRI and electrodiagnostic study. Electromyography and clinical neurophysiology, 43(1), 57-64.
- Narasimhan P, Sklar R, Murrell M, Swanson RA, Sharp FR. Methylmalonyl-CoA mutase induction by cerebral ischemia and neurotoxicity of the mitochondrial toxin methylmalonic acid. J. Neurosci. 16, 7336–7346 (1996).
- Qureshi GA, Qureshi AA, Devrajani BR, Chippa MA, Syed SA. Is the deficiency of vitamin B12 related to oxidative stress and neurotoxicity in Parkinson’s patients? CNS Neuro. Disord. Drug Targets 7, 20–27 (2008).
- Scalabrino, G. (2016). Clarifying the Molecular Basis of Cobalamin (Vitamin B12) Neurotrophism. J Headache Pain Manag, 1, 2.
- Scalabrino G, Veber D, Tredici G (2014) Relationships between cobalamin, epidermal growth factor, and normal prions in the myelin maintenance of central nervous system. Int J Biochem Cell Biol 55: 232-241.
- Miller JW. Vitamin B12 deficiency, tumor necrosis factor-alpha, and epidermal growth factor: a novel function for vitamin B12? Nutr Rev 2002;60:142–4.
- Watanabe TE: Ultrahigh dose Methylcobalamin prometes nerve Regeneration in experimental acrylamid neuropathy. J Neurol Sci 1994, 12(2):140–143.
- Hobbenaghi, R., Javanbakht, J., Hosseini, E., Mohammadi, S., Rajabian, M., & Moayeri, P. (2013). Neuropathological and neuroprotective features of vitamin B 12 on the dorsal spinal ganglion of rats after the experimental crush of sciatic nerve: an experimental study. Diagnostic pathology, 8(1), 1.
- Liao W-C, Wang Y-J, Huang M-C, Tseng G-F (2013) Methylcobalamin Facilitates Collateral Sprouting of Donor Axons and Innervation of Recipient Muscle in End-to-Side Neurorrhaphy in Rats. PLoS ONE 8(9): e76302.
- Kiyoshi Okada, Hiroyuki Tanaka, Ko Temporin, Michio Okamoto, Yusuke Kuroda, Hisao Moritomo, Tsuyoshi Murase, Hideki Yoshikawa, Methylcobalamin increases Erk1/2 and Akt activities through the methylation cycle and promotes nerve regeneration in a rat sciatic nerve injury model, Experimental Neurology, Volume 222, Issue 2, April 2010, Pages 191-203
- Tanaka, H. (2013). [Old or new medicine? Vitamin B12 and peripheral nerve neuropathy]. Brain and nerve= Shinkei kenkyu no shinpo, 65(9), 1077-1082.
- Sun, H., Yang, T., Li, Q., Zhu, Z., Wang, L., Bai, G., … & Wang, W. (2012). Dexamethasone and vitamin B12 synergistically promote peripheral nerve regeneration in rats by upregulating the expression of brain-derived neurotrophic factor. Arch Med Sci, 8(5), 924-930.
- Izumi, Y., & Kaji, R. (2008). Clinical trials of ultra-high-dose methylcobalamin in ALS. Alternative Medicine Review, 13(1), 75-76.
- Sakly, G., Hellara, O., Trabelsi, A., & Dogui, M. (2004). [Reversible peripheral neuropathy induced by vitamin B12 deficiency]. Neurophysiologie clinique= Clinical neurophysiology, 35(5-6), 149-153.
- Ide H, Fujiya S, Asanuma Y, Tsuji M, Sakai H, Agishi Y. Clinical usefulness of intrathecal injection of methylcobalamin in patients with diabetic neuropathy. Clin Ther. 1987;9(2):183-92.
- Wellmer, J., Sturm, KU., Herrmann, W. et al. Orale Vitamin-B12-Substitution bei funikulärer Myelose. Nervenarzt (2006) 77: 1228.
- Bolaman Z, Kadikoylu G, Yukselen V et al. (2003) Oral versus intramuscular cobalamin treatment in megaloblastic anemia: a single-center, prospective, randomized, open-label study. Clin Ther 25: 3124–3134
- Buttler CC, Vidal-Alaball J, Cannings-John R et al. (2006) Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency: a systematic review of randomized controlled trials. Fam Pract 23: 279–285
- Dror, D. K., & Allen, L. H. (2008). Effect of vitamin B12 deficiency on neurodevelopment in infants: current knowledge and possible mechanisms. Nutrition reviews, 66(5), 250-255.
- Baatenburg de long R, Bekhof J, Roorda R, Zwart P. Severe nutritional vitamin deficiency in a breast-fed infant of a vegan mother. Eur J Pediatr. 2005;164:259-260.
- Campbell CD, Ganesh J, Ficicioglu C. Two newborns with nutritional vitamin B 12 deficiency: challenges in newborn screening for vitamin B 12 deficiency. Haematologica. 2005;90(12 Suppl):ECR45.
- Casella EB, Valente M, de Navarro JM, Kok F. Vitamin B 12 defi- ciency in infancy as a cause of developmental regression. Brain Dev. 2005;27:592-594.
- Codazzi D, Sala F, Parini R, Langer M. Coma and respiratory failure in a child with severe vitamin B(1 2) deficiency. Pediatr Crit Care Med. 2005;6:483-485.
- Rosenblatt DS, Whitehead VM. Cobalamin and folate deficiency: acquired and hereditary disorders in children. Semin. Hematol. 36(1), 19–34 (1999).
- von Schenck, U., Bender-Götze, C., & Koletzko, B. (1997). Persistence of neurological damage induced by dietary vitamin B-12 deficiency in infancy. Archives of disease in childhood, 77(2), 137-139.
- Stephen M. Graham, Otto M. Arvela, Graham A. Wise, Long-term neurologic consequences of nutritional vitamin B12 deficiency in infants, The Journal of Pediatrics, Volume 121, Issue 5, 1992, Pages 710-714, ISSN 0022-3476,
- Bell, D. S. (2010). Metformin-induced vitamin B12 deficiency presenting as a peripheral neuropathy. Southern medical journal, 103(3), 265-267.
- Yaqub, B. A., Siddique, A., & Sulimani, R. (1992). Effects of methylcobalamin on diabetic neuropathy. Clinical neurology and neurosurgery, 94(2), 105109-108111.
- Li G. Effect of mecobalamin on diabetic neuropathies: Beijing Methycobal Clinical Trial Collaborative Group. Zhonghua Nei Ke Za Zhi 1999;38:14–17
- Dominguez JC, Ng AR, Damian LF. A prospective, open label, 24-week trial of methylcobalamin in the treatment of diabetic polyneuro
- Sun Y, Lai MS, Lu CJ. Effectiveness of vitamin B12 on diabetic neuropathy: systematic review of clinical controlled trials. Acta Neurol Taiwan 2005;14:48–54
- Talaei A, Siavash M, Majidi H, Chehrei A. Vitamin B12 may be more effective than nortriptyline in improving painful diabetic neuropathy. Int J Food Sci Nutr 2009;5:71–76
- Hermann L, Nilsson B, Wettre S. Vitamin B12 status of patients treated with metformin: a cross-sectional cohort study. Br J Diabetes Vasc Dis 2004;4:401–406
- Qureshi SA, Ainsworth A, Winocour PH. Metformin therapy and assessment for vitamin B12 deficiency: is it necessary? Pract Diabetes 2001;28:302–304
- Singh AK, Kumar A, Karmakar D, Jha RK. Association of B12 deficiency and clinical neuropathy with metformin use in type 2 diabetes patients. J Postgrad Med 2013;59:253–257
- Bauman, W. A., Shaw, S., Jayatilleke, E., Spungen, A. M., & Herbert, V. (2000). Increased intake of calcium reverses vitamin B12 malabsorption induced by metformin. Diabetes care, 23(9), 1227-1231.
- Filippo TS, Holder WD Jr. Neurologic degeneration associated with nitrous oxide anesthesia in patients with vitamin B12 deficiency. Arch Surg. 1993 Dec;128(12):1391-5. Review. PubMed PMID: 8250714
- Marié R, Le Biez E, Busson P, et al. Nitrous Oxide Anesthesia–Associated Myelopathy. Arch Neurol. 2000;57(3):380-382. doi:10.1001/archneur.57.3.380.
- Birch, C. S., Brasch, N. E., McCaddon, A., & Williams, J. H. (2009). A novel role for vitamin B 12: Cobalamins are intracellular antioxidants in vitro. Free Radical Biology and Medicine, 47(2), 184-188.
- Lee, Y. J., Wang, M. Y., Lin, M. C., & Lin, P. T. (2016). Associations between Vitamin B-12 Status and Oxidative Stress and Inflammation in Diabetic Vegetarians and Omnivores. Nutrients, 8(3), 118.
- Suarez-Moreira, E., Yun, J., Birch, C. S., Williams, J. H., McCaddon, A., & Brasch, N. E. (2009). Vitamin B12 and redox homeostasis: cob (II) alamin reacts with superoxide at rates approaching superoxide dismutase (SOD). Journal of the American Chemical Society, 131(42), 15078-15079.
- van der Kuy PH, Merkus FW, Lohman JJ, ter Berg JW, Hooymans PM. Hydroxocobalamin, a nitric oxide scavenger, in the prophylaxis of migraine: an open, pilot study. Cephalalgia. 2002 Sep;22(7):513-9
- Wheatley, C. (2007). Cobalamin in inflammation III—glutathionylcobalamin and methylcobalamin/adenosylcobalamin coenzymes: the sword in the stone? How cobalamin may directly regulate the nitric oxide synthases. Journal of nutritional & environmental medicine, 16(3-4), 212-226.
- Ling, C. T., & Chow, B. F. (1953). The effect of vitamin B12 on the levels of soluble sulfhydryl compounds in blood. Journal of Biological Chemistry, 202, 445-456.

